Loiasis And Onchocerciasis: Health Implications And Clinical Presentations To Man

Physical Presentation Of The Loa Loa Infection
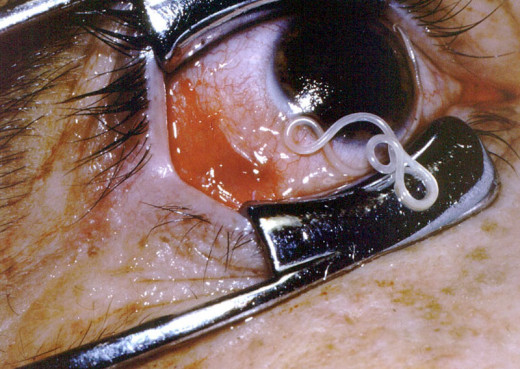
Loiasis
Loa loa is prevalent in west and central Africa and this is commonly known as the African eye worm. The adult worms migrate in the subcutaneous tissues of several parts of the body including the eyes. Adult female measures 70 mm in length whereas the male measures only 30 mm. The thickness ranges from 0.3 to 0.4 mm. They live for 10 to 15 years. Sheathed microfilaria are produced and these appear in the blood during day time. This infection is transmitted by Chrysops (C. silacca and C. dimidiate) which act as vectors. In many endemic areas monkeys from the reservoir.
The disease manifests as Calabar swellings which are recurrent localized allergic inflammatory swellings. The swellings may overlie the adult worms at times. They commonly appear over the limbs or trunk. When the eyes are affected, intense lacrimation and pain may result. Endomyocardial fibrosis is more prevalent in areas endemic for loiasis. Rarely meningoencephalitis may be caused by this parasite. The examination of CSF may show the parasites. Treatment conssits of the administration of diethyl carbamazine which kills both adults and microfilaria. The dose is 6 mg/Kg given for 14 days.
Physical Presentation Of The African River Blindness

Infectious Diseases

Onchocerciasis (African River Blindness)
This is a cutaneous form of filariasis caused by Onchocerca volvulus prevalent throughout tropical Africa, Mexico, Guatemala, Eastern Venezuela and Northern Brazil. This disease has not been identified in India.
The female worm measures 3 to 5 cm and the male is 2 to 3 cm in length. The adult worms lie tangled together in the subcutaneous nodules and they live for 7 to 15 years. The microfilaria, which are unsheathed, are widely distributed in the adjacent skin. The vectors are female black flies belonging to the genus Simulium.
Clinical Manifestations: The adult worms give rise to subcutaneous nodules which are 0.5 to 5cm in diameter. These are firm, nontender, freely movable and are most commonly seen around the head and shoulders or the pelvic girdle. The skin manifestations are intensely itchy lesions which in the early stages are seen as papulo-erythematous rashes. Later, the skin becomes thickened, hyperkeratotic (crocodile skin) and depigmented. The penis and scrotum may show elephantoid changes.
Ocular lesions develop especially if the adults are numerous over the head and neck. These are punctuate ketatitis, iridocyclitis and rarely choroidoretinitis, all of which ultimately lead to blindness.
Diagnosis: Demonstration of microfilaria in the skin shavings or skin snips taken from the affected area, or the adults in biopsy of the nodules, establishes the diagnosis. Complement fixation test is available for serological diagnosis.
Treatment: The microfilaria are rapidly destroyed by diethyl carbamazine but the drug is ineffective on adult worms. The drug is started in a low dose and gradually worked up to 100 mg given thrice daily for 7 to 10 days. Severe allergic reactions may complicate the initial phase of therapy. Ocular lesions have to be treated with mydriatics and topical steroid applications. The adult worms are removed by excision of nodules wherever they are accessible. The drug of choice is suramin, intravenously in doses of 1g weekly for five to siex weeks. Major toxic effects of suramin are renal damage which is manifested early as proteinuria. Control of infection in endemic areas is achieved by antivector measures, mass therapy of cases and personal prophylaxis.
© 2014 Funom Theophilus Makama


