Clinical Features, Complications, Prognosis And Treatment Of Mitral Regurgitation

Reverse Flow In Regurgitation

Clinical Cardiology

Clinical Presentation Of Mitral Regurgitation
This depends on the severity of MR. Symptoms include palpitation, exertional dypsnea, weakness and fatigue. The only abnormality in mild cases is the presence of a pansystolic murmur over the cardiac apex. In moderate and severe cases, other features develop. The pulse of severe MR is described as pseudocollapsing with the pulse pressure above 40 mmHg and it is of short duration. Left ventricular enlargement is evidenced by the forcible apex beat which is shifted down and out. The characteristic murmur of MR is medium to high pitched pansystolic murmur heard best over the apex beat. In cases where the anterior mitral leaflet is damaged, the murmur is conducted to the axilla because the direction of the regurgitant stream from the left ventricule is towards the body of the left atrium. In cases with posterior leaflet involvement, the murmur is conducted to the anterior chest and to the right upper sterna border because the regurgitant stream is directed towards the inter-artrial septum. In moderate and severe cases, the murmur occupies the whole of systole and is moderately loud in intensity.
Such cases show evidence of left ventricular enlargement. A left ventricular third heart sound is common. A mid-diastolic murmur which is decrescendo in character may be heard over the apex beat following the third heart sound. The third heart sound and the diastolic murmur indicate increased flow across the mitral valve. In severe cases evidence of pulmonary arterial hypertension may be evident.
Electrocardiogram in mild case is normal. In moderate and severe cases, left ventricular hypertrophy and left atrial enlargement are seen. The ECG may also help in determining the etiology of MR.
Chest X-ray: Moderate and severe cases show left ventricular type of cardiac enlargement. The left atrium is also enlarged. Very large left atrium (giant left atrium) is met with in some of the severe cases. Evidence of pulmonary venous and arterial hypertension may be seen.
Echocardiography is helpful in the assessment of the etiology and severity of MR. Cardiac catheterization and left ventriculography are the methods of choice for the exact quantification and assessment of the hemodynamic abnormality.
Complication
These include congestive heart failure, atrial fibrillation and infective endocarditis. It should be remembered that MR is one of the best tolerated lesions and therefore, may remain asymptomatic for several years.
Course and prognosis
Mild MR may remain asymptomatic. Unless complicated by infective endocarditis, it may not progress further. Moderate and severe cases become symptomatic. Development of pulmonary hypertension is relatively slow in MR and the pulmonary pressure tends to be lower than that seen in mitral stenosis. In Africa where rheumatic heart disease is still rampant, severe grades of pulmonary arterial hypertension are seen in MR. Severe MR usually progresses and results in congestive heart failure. Atrial fibrillation may develop as a complication, but embolic episodes are rarer compared to mitral stenosis.
Acute severe MR is almost always a medical emergency and even with emergency treatment, the mortality is high.
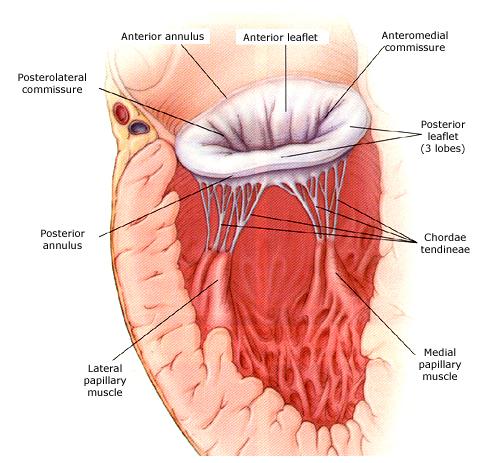
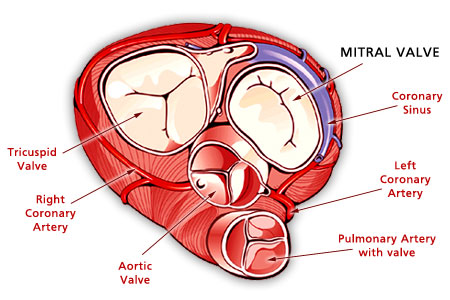
The Mitral Valve In Details
Treatment
Treatment
Mitral regurgitation with symptoms of pulmonary veinous hypertension has to be treated with diuretics. Congestive heart failure has to be managed before submitting the patient to mitral valve surgery.
The ideal treatment for correcting the abnormality is mitral valve replacement. In moderate and severe cases, valve replacement has to be considered as an elective procedure after correcting the complications if any. In acute severe MR, which is not controlled by medical treatment, valve replacement should be considered as an emergency procedure to save life.
Combination of mitral stenosis and incompetence
In a large number of cases of rheumatic affection of the mitral valve, there is a combination of mitral stenosis and incompetence. Either may predominate. The clinical findings are modified depending upon the severity of each lesion.
© 2014 Funom Theophilus Makama




