Addisonian Pernicious Anemia And Other Congenital Causes Of Anemia

Pernicious Anemia Patient

Introduction
This disorder is also known as just pernicious anemia or Biermer’s anemia.
Etiology: Pernicious anemia is common among the Caucasian population, but is very rare in Indian and African subjects. It is found more often in the older age groups and only rarely before 30 years of age. It may be familial and affects both sexes. Antibodies directed against the gastric parietal cells are present in the serum in 85- 90% of cases and antibodies against intrinsic factor are demonstrable in the serum as well as in the gastric juice in a smaller proportion of cases. Autoimmune mechanisms are probably responsible for their presence. The gastric mucosa undergoes atrophy resulting in the absence of intrinsic factor and gastric acid. Dietary vitamin B12 is not absorbed. Other disorders like myxedema, Addison’s disease, thyrotoxicosis, Hashimoto’s disease and vitiligo may occur along with pernicious anemia. Carcinoma of the stomach develops in 4% of cases when followed up for long periods.
Diarrhea: One Of The Symptoms Of Pernicious Anemia


Clinical Features And Manipulations
Clinical features
The onset is insidious. In addition to symptoms of anemia, special features include soreness of the tongue, paraesthesia of hands and feet, diarrhea and yellowish tinge of skin and mucous membranes. The tongue is atrophic. Spleen is palpable in 25% of cases. Psychiatric symptoms are common. Spinal cord lesions take the form of subacute combined degeneration in which varying combinations of posterior column and pyramidal tract dysfunction are encountered. If left untreated, the disease follows a prolonged course, ending fatally due to severe anemia or its complications.
Laboratory findings
Erythrocytes are macrocytic with marked anisopoikilocytosis. The bone marrow is megaloblastic. In a florid case, the hemoglobin isusually below 7 g/dl. Leucopenia and thrombocytopenia are common. Gastric analysis shows histamine fast achlorhydria and absence of intrinsic factor (achylia gastric). Serum vitamin B12 is below 80 pg/ml. Serum and red cell folate are normal. Serum Iron levels are elevated.
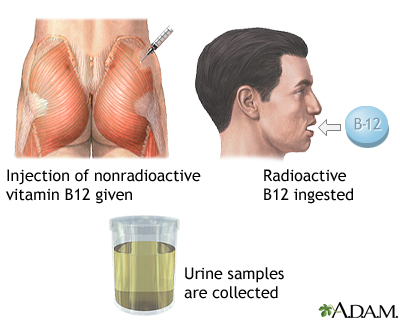
Defect of absorption of vitamin B12 and its correction by addition of intrinsic factor present in normal gastric juice can be demonstrated by Schilling’s test using radioactive vitamin B12. Parietal cell antibodies which are detectable in the serum are helpful in diagnosis.
Therapy
In severe cases, where the hemoglobin is below 5g/dl, transfusion of packed erythrocytes may be required. Specific therapy is to give hydroxocobalamin 1000 ug intramuscularly every week till Hb level becomes normal. Reticulocyte response is noticed within 2 to 3 days of the first injection. Folic acid is contraindicated since it is known to precipitate the neurological complications, if administered alone.
Treatment Plan Of Pernicious Anemia
Maintenance
Subjects with pernicious anemia should receive lifelong supplementation of parenteral vitamin B12, 1000 ug every month.
Congenital megaloblastic anemias: Though in the vast majority of cases of pernicious anemia, the defect in intrinsic factor is an acquired one, it can be congenital in some rare cases.
Congenital intrinsic factor deficiency: In this condition, the gastric histology and secretions are normal except for the absence of intrinsic factor.
Congenital deficiency of transcobalamin II (TCII) also causes megaloblastic anemia. In this condition, the serum level of vitamin B12 is normal, but since it is bound to transcobalamin I, it is not available for hematopoiesis.
© 2014 Funom Theophilus Makama


 Factor Easily Explained")


